Developmental Dysplasia of the Hip
within 72 hours of being born, and again at 6 to 8 weeks of age.
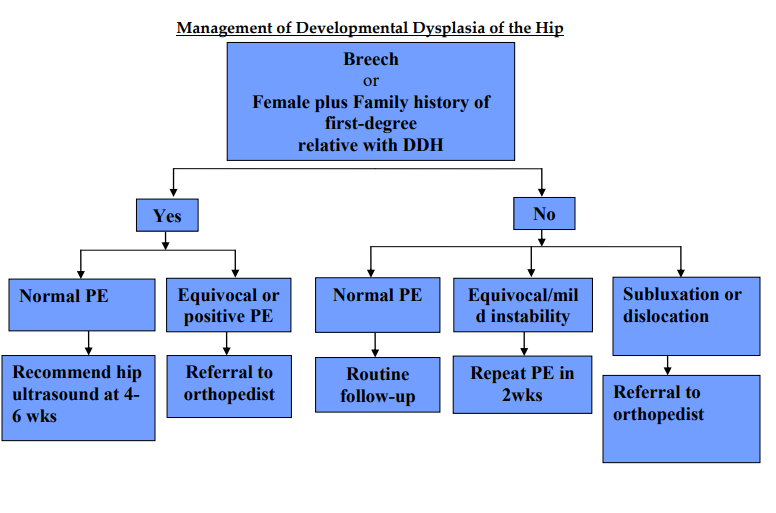
Babies should also have an ultrasound scan of their hip between 4 and 6 wks if:
- There have been childhood hip problems in your family.
- your baby was born in the breech position (feet or bottom downwards) after 28 weeks of pregnancy.
If you have had twins or multiples and 1 of the babies was in the breech position, each baby should have an ultrasound scan of their hips by the time they’re 4 to 6 weeks old.

Babies diagnosed with DDH early in life are usually treated with a fabric splint called a Pavlik harness.
This secures both of your baby’s hips in a stable position and allows them to develop normally.
The harness needs to be worn constantly for 6 to 12 weeks and should not be removed by anyone except a health professional.
If the femoral head is dislocated, hip reduction is easier within the first months of life. In a child aged under six months, the Pavlik harness is the most used orthosis for reducing a dislocated or subluxated hip and is usually the first line of treatment.
The Pavlik harness should be worn to allow hip abduction between 30° (less abduction allows hip dislocation) and 60° (higher abduction increases risk of AVN).
It is not recommended in large children, in patients older than eight months, when the hip needs excessive flexion to keep reduction or when the hip is very unstable with adduction.
Whenever a Pavlik harness is used, the hip should be reduced within the first three to four weeks.
It can be confirmed either by physical examination or echography. If the hip is reduced within the harness, it will be kept until the hip stabilises and the acetabulum normalises.
If not, harness treatment should be suspended because of the risk of AVN. The success rate of a Pavlik harness in reducing an Ortolani-positive hip is in the range of 85% to 92%. Risk factors for failure are: irreducible hip with Ortolani manoeuvre; inverted labrum; high β angle; insufficient coverture of the head; acetabular index >36°; and bilateral dislocation.
If a force closed reduction is attempted or a dislocated hip is maintained within the cast, AVN could occur.66 MRI is useful to assess reduction within the cast. On the other hand, open reduction has also been related to AVN. Some authors believe that AVN after an open reduction is higher when the ossification nucleus of the femoral head is still absent in X-rays. Therefore, delaying open reduction until complete ossification of the femoral head can decrease the risk of AVN. However, the later the hip is reduced, the higher the risk of multiple surgeries.
Once a stable reduction is obtained by closed or open means, it should be stabilised for three months in a spica cast.
classification
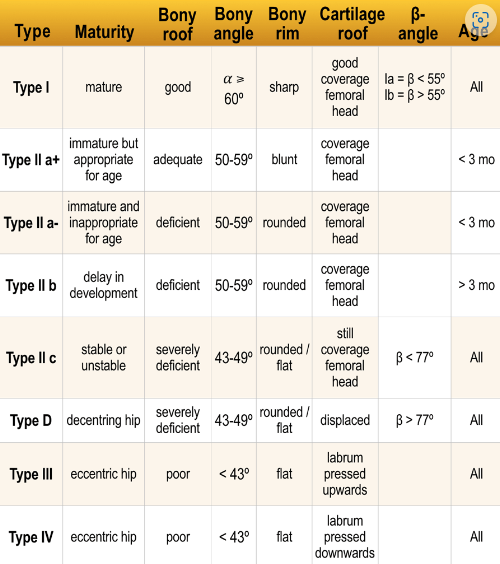
GRAF classification:
- Alpha angle-angle between bony acetabulum and Illium (Normal > 60 degrees)
- Beta angle-angle between labrum and ileum (Normal < 55 degrees)
Based on these angles, DDH is classified into four types.
X-ray: anteroposterior (AP) of the pelvis – lines of mensuration:
- Hilgenreiner’s line: a horizontal line through the right and left triradiate cartilage, head of the femur should be inferior to this line. (Figure 1)
- Perkin’s line: Perpendicular line to Hilgenreiner’s line through a focus at the lateral side of the acetabulum. The femoral head should be medial to this line. (Figure 2)
- Shenton’s line: Smooth arc that connects the femoral neck to the superior margin of the obturator foramen. Any disruption indicates an abnormality. (Figure 3)
- Acetabular index: the intersection between Hilgenreiner’s line and a line drawn tangential to the lateral ossific margin of the roof of the acetabulum. The normal index is less than <35 degrees at birth and <25 degrees at age one. (Figure 4)
- The center-edge angle of Wiberg: Formed by Perkin´s line and a line coming from the center of the femoral head to the lateral edge of the acetabulum. This measurement is reliable in patients older than 5 years old. Values should be > 20 degrees.
The descriptions used in the Graf method assume the standard projection is an ultrasound image of the hip that is set up as a vertical right hip AP view.
- type I
- centered hip
- alpha angle >60° (normal)
- type Ia: beta angle <55°
- type Ib: beta angle >55°
- type II
- centered hip
- type IIa (physiologically immature): alpha angle 50-59° (<3 months)
- type IIb: alpha angle 50-59° (>3 months)
- type IIc
- alpha angle 43-49°
- beta angle <77°
- type D (“about to decentre”)
- alpha angle 43-49°
- beta angle >77°
- type III
- decentred hip
- alpha angle: not measured in a decentred hip
- cartilage roof pushed partly upwards (cephalad), partly downwards (caudal)
- perichondrium goes upward (ultrasound image set as right hip AP)
- type IIIa: no echos in cartilaginous roof
- type IIIb: echos in cartilaginous roof due to structural alteration and damage
- type IV
- decentred hip
- alpha angle: not measured in a decentred hip
- cartilage roof pushed entirely downwards (cephalad)
- perichondrium goes horizontal (ultrasound image set as right hip AP)
- the hyaline cartilage of the lateral edge of the acetabulum along with fibrocartilaginous labrum is interposed between the femoral head and the acetabulum
Criteria for DDH has been established for static imaging (Graf classification)
Up to the age of 3 months (13 weeks) an alpha angle below 60 degrees is acceptable.
A neonate can even start with an alpha angle of 50 degrees provided that the angle gradually reaches the 60 degrees by the age of 12 weeks.
At the age of 3 months the decision has to be made whether the hip is normal or not.
Evidently if a neonate starts with an alpha angle of 60 degrees than everything is o.k. and no follow up is necessary.
Treatment
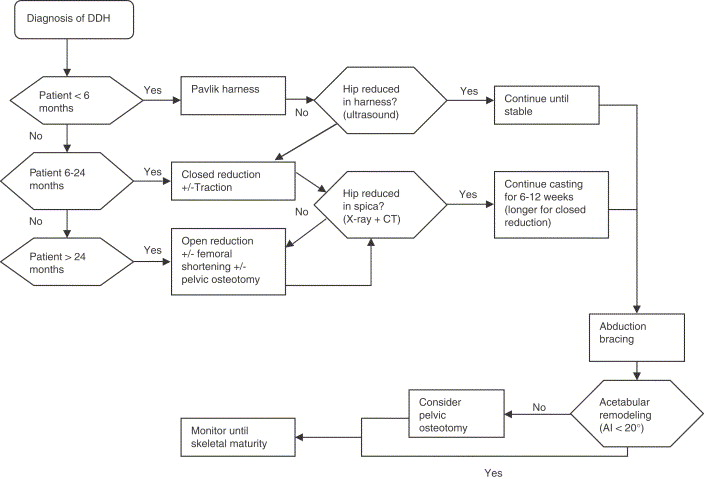
0 to 4 Weeks
- Mild instability without a dislocatable hip can be watched.
- Early referral to an orthopedic surgeon experienced treatment of DDH will be optimal if the hips are dislocatable. The application of abduction splints (Pavlik harness) will be up to the orthopedic surgeon who manages it. But a study done by Larson JE et al. concluded waiting up to 30 days before initiation of treatment shows no significant difference in the outcome.
1 to 6 Months
Abduction devices like Pavlik harness, Von Rosen splint, Lausanne-developed abduction brace, Ilfeld orthosis, and Frejka pillow can be tried. Pavlik harness is the widely used device for DDH. It consists of an anterior strap that flexes the hip at 90 degrees and prevents extension, posterior strap to prevent adduction. Its worn 23 hours per day for at least six weeks or until the hip is stable. The US of the hip is done every 3- 4 weeks to monitor the position of the femoral head. The success rate is about 90 % for Barlow’s positive hip.
The failure rate is high with the following conditions: Ortolani positive hip, initiation of treatment after seven weeks, multigravida, foot deformity, and male sex.
If the hips are not reduced by three weeks, semi-rigid, non-flexible abduction devices like Ilfed orthosis to keep the hip in abducted position can be tried in a study by Sankar et al. 82 % success rate with Ilfed orthosis after Pavlik harness failure.
6 to 18 Months
For infants who are diagnosed with DDH at this age or patients who failed with abduction devices, closed reduction with hip spica cast is preferred. Under general anesthesia (GA), the hip is placed in 90-100 degrees flexion and 40-50 degrees abduction. The failure rate is about 13.6 %.
The main complication is avascular necrosis of the head. CT or MRI is needed to confirm the position of the hip position. In a study by Gornitzky AL et al., MRI with contrast can identify perfusion abnormalities following closed reduction, thus preventing AVN.
18 Months to 8 Years
Open reduction is preferred for children diagnosed with DDH over 18 months and infants who failed closed reduction. Open reduction can be used to correct anatomical abnormalities like inverted labrum, neolimbus, pulvinar, hypertrophied ligamentum trees. Capsulorrhaphy and release of tight iliopsoas tendon can also be done. The two preferred approaches are anterior (Smith-Peterson) and medial. Medial is less invasive, but anterior is classical and will help correct most of the anatomical abnormalities. A femoral shortening osteotomy can be added to children if needed. The main complication is AVN. After open reduction, a spica cast applied and reduction is confirmed with CT or MRI.
Acetabular Dysplasia
Children with shallow or vertical acetabulum lead to osteoarthritis due to edge loading. Patients presenting with acetabular dysplasia up to age 5, without dislocation can be treated with part-time or full-time abduction orthosis.
After age 5, pelvic osteotomies (Salter, Pemberton, and Dega) use a single cut to increase anterior or anterolateral coverage. If the patient has an open triradiate cartilage center, triple cut (triple innominate osteotomy) can be performed.
Salvage pelvic osteotomies: Shelf procedure is indicated for patients >8 years old with a subluxated femoral head. By placing an extra-articular buttress of bone to the lateral weight-bearing aspect of the acetabulum. Chiari procedure is indicated for patients with inadequate femoral head coverage with a concentric reduction that cannot be obtained. It medializes the acetabulum via iliac osteotomy.
Adolescent/Adult Hip Preservation Surgery
Patients who are presenting with hip pain and with shallow acetabulum (radiographic femoral head undercoverage), and closed triradiate cartilage but without signs of hip degeneration can be treated with a periacetabular osteotomy (PAO). Bernese PAO is a technique in which multiple cuts are made to modify and reorient acetabular cartilage while maintaining an intact posterior column.